Presentation: View Royal Community Primary Care Attachment Clinic
A concept proposal by Aroga Lifestyle Medicine for a community-governed primary care clinic to address the shortage of family doctors in View Royal.
View Royal Community Primary Care Attachment Clinic
Primary Care is for Everyone
Concept Paper for Discussion
PREPARED BY: Aroga Lifestyle Medicine
DATE: 2 June 2026
STATUS: Public Releasable
A Growing Primary Care Crisis in View Royal
12,782*: View Royal residents and growing
~35%: Estimated residents currently unattached
~4,500+: Residents without a family care provider
Unattached residents rely on emergency departments, urgent care centres, walk-in clinics and paid services — driving up system costs and congestion.
Reduced preventative care leads to poorer chronic disease management and worse long-term health outcomes for residents.
Military families who frequently move find greater challenges securing primary care.
*BC Stats 27 May 2025 Update
A Community-Governed Solution
The proposed View Royal Community Primary Care Attachment Clinic would operate as an independent non-profit society under the BC Societies Act — attaching unattached residents through a sustainable, team-based model aligned with provincial and Island Health priorities.
Or
This may work as a Partnership Agreement as defined by the Community Charter.
- Municipal representation on a community Board
- Non-profit society — not a municipal service
- Physician & Nurse Practitioner compensation via provincial billing
- Aligned with Island Health and PCN priorities
Team-Based Primary Care — 2,500 sq. ft.
- Family Physicians & NPs: Longitudinal attachment-based care, preventative health, and chronic disease management.
- Registered Nurses: Clinical support, triage, and care coordination embedded within the care team.
- Mental Health Supports: Integrated mental health access within primary care — reducing specialist wait times.
- Allied Health: Social work, dietitian, and other allied professionals as part of a full-spectrum team.
- Virtual Care Integration: In-person and virtual care appointments for improved access and patient convenience.
- Care Coordination: Administrative and referral support to connect patients to the right services efficiently.
Who We Serve and How
Clinical Services
- Longitudinal family and preventative care
- Chronic disease management
- Senior’s care and women's health
- Mental health supports
- Culturally informed care pathways
- Attachment for Health Connect Registry residents
Priority Populations
- Unattached View Royal Residents: Currently registered in BC Health Connect Registry
- Seniors & Vulnerable: Prioritised for complex care and chronic conditions
- First Responders: View Royal Fire Service members and Westshore RCMP
- Military Families & Veterans: CAF veterans and military families
Six Pillars of the Initiative
- Primary Care Attachment: Improve attachment rates for View Royal residents on the Health Connect Registry.
- Long-Term Sustainability: A financially viable, operationally independent healthcare delivery model.
- Community Health Outcomes: Preventative care, chronic disease management, and continuity of longitudinal care.
- Healthcare System Support: Reduce non-emergent emergency department utilization across the region.
- Regional Collaboration: Partner with Island Health, Division of Family Practice, and community organizations.
- First Responder: Taking care of those who take care of us and keep our community safe.
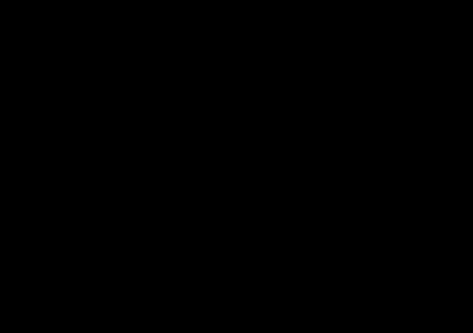
Community Board Governance Structure
Board Composition
- Town of View Royal
- Military / First Responders
- Healthcare Professionals
- Community Representatives
- Legal / Financial Expertise
- Healthcare System Advisors
The Town's role focuses on community leadership, partnership facilitation, and strategic oversight — not direct clinical operation.
Clinical liability and professional licensing risks remain with the non-profit board, medical director and individual practitioners.
Legal and Financial expertise will be included on the Board to protect society’s viability.
What View Royal Is Being Asked to Contribute
- ~$770K: One-time startup contribution for renovation
- $110K–$130K: Annual facility lease participation
- $8.61–$10.17 per yr: Per resident annually
- The Town would NOT directly fund physician compensation.
- Physicians bill through provincial compensation systems. NPs funded via Island Health / PCN allocations.
- Municipal role: startup facilitation, facility participation, governance, and operational stabilization. Long-term clinical funding remains a provincial responsibility.
- The Town is positioned as a community health enabler — not a healthcare operator.
- If Council directs staff to proceed, a detailed Class C cost estimate and feasibility assessment could support future federal and partner funding applications.
Estimated One-Time Capital Investment
| Item | Detail | Estimated Amount |
|---|---|---|
| Improvements / build-out | $225/sq. ft. net cost | $562,500 |
| Equipment and furnishings | 8 exam rooms + waiting + other | $190,000 |
| Legal and startup costs | Incorporation, professional fees | $25,000 |
| Total CAPEX and Startup | $777,500 | |
| View Royal Capital Support | $770,000 | |
| Net Shortfall | ($7,500) |
Two-Year Financial Summary
Year 1
| Item | Total |
|---|---|
| Total Clinical Revenue | $539,400 |
| Physician Fees (COGS) | $316,800 |
| Gross Margin | $222,600 |
| Total Operating Expenses | $351,857 |
| View Royal Contribution | $130,000 |
| Net Result | $743 |
Year 2
| Item | Total |
|---|---|
| Total Clinical Revenue | $1,029,000 |
| Physician Fees (COGS) | $567,000 |
| Gross Margin | $462,000 |
| Total Operating Expenses | $559,787 |
| View Royal Contribution | $130,000 |
| Net Result | $32,213 |
Projections assume patient attachment ramping from 75 patients (Month 1) to 3,625 patients by end of Year 2. Physician compensation funded through provincial billing.
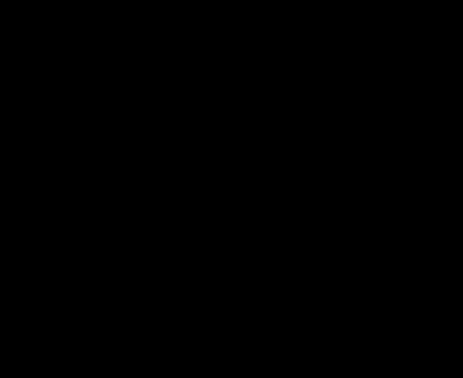
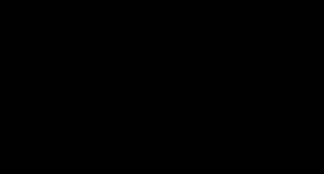
Patient Attachment Ramp — Years 1 and 2
Staffing FTE Ramp
| Period | MD | NP | Total |
|---|---|---|---|
| Y1, M1–5 | 1.0 | 0.5 | 1.5 |
| Y1, M6–12 | 1.5 | 1.0 | 2.5 |
| Y2, M1–6 | 2.0 | 1.5 | 3.5 |
| Y2, M7–12 | 2.5 | 2.0 | 4.5 |
- Year 1 Target: 1,250 residents
- Year 2 Target: 3,600 residents
Building a Collaborative Funding Model
- Island Health / PCN: NP allocations, allied health support, attachment program integration, operational and systems grants.
- First Responders: Attachment pathway for View Royal Fire Rescue members and Westshore RCMP.
- CFB Esquimalt / DND / VAC: Attachment pathways for veterans, and military families. Potential federal funding support.
- Grants & Philanthropy: Startup and tenant improvement grants, equipment funding, innovation and community wellness funding.
- Victoria Foundation & Legions: Community fundraising, service organization support, and local philanthropic contributions.
- Property / Landlord: Tenant improvement allowances, reduced lease escalation, phased rent commencement.
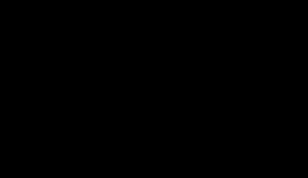
Measurable Impact for View Royal Residents
Community Attachment Context
- Total View Royal Residents: 12,782
- Estimated Unattached (35%): 4,500
- New Residents by 2030: 2,000
- Veterans / Military Families: 2,000
- Total Attachment Target: 8,500
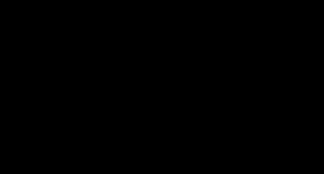
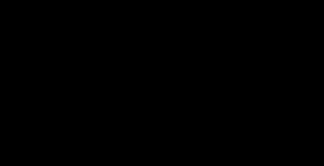
Illustrative Targets
- Year 1 Attachment: 1,250 residents
- Year 2 Attachment: 3,600 residents
- Priority Groups: Seniors, medically vulnerable
- Military & Veterans: CAF families, first responders, Westshore communities
- ED Diversion: Measurable reduction in non-emergent ED visits
Recommended Next Steps
This concept paper is submitted to View Royal Municipal Council for consideration and direction on proceeding with exploratory next steps.
- Establish Exploratory Discussions — Island Health, Division of Family Practice, Ministry of Health, Federal Grant Funding, and clinical partners.
- Develop Foundational Documents — Governance framework, Class C Estimate, Non-profit incorporation, preliminary financial model, and feasibility analysis.
- Confirm Partnership Capacity — Staffing partners, clinical leadership, and facility requirements.
- Prepare Full Business Plan — Detailed plan, comprehensive funding strategy, and phased implementation roadmap.
- Report Back to Council — Feasibility findings, funding pathways, governance recommendations, and implementation options.
Document Images
(5)
Flowchart illustrating the governance hierarchy from the BC Societies Act Non-Profit Society down to Patient Care Delivery
Bar chart showing the projected patient attachment growth from Year 1 Month 1-5 to Year 2 Month 7-12
Bar chart depicting the community attachment context and target populations
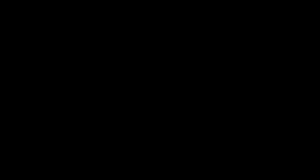
Diagram displaying outcome targets for patient attachment and clinical priorities
Numbered timeline graphic of the five recommended next steps